Overnight Camp & The Brain: The Hidden Benefits of a Summer Spent in Cabins
By Rachel Kimball

Introduction:
Some parents choose to send their kids off to sleep-away camp year after year. As days are filled with sailing, waterskiing, dancing, and bunk time, it makes us wonder: other than the fun that comes out of the several weeks spent away from home, how does it benefit these kids? This question can be answered in many ways ways, but one key component in how overnight camp benefits campers has to do with what the MAPP Scholars focus on most: the brain!
Staying Active & The Brain:
I spent eight summers at a camp in NH, and it is no joke that my watch tracked 20,000+ steps a day. From running to activities, to swimming laps in the pool, to dancing and kickball, kids are more active at camps than anywhere else. As mentioned in our Instagram posts, there is a very clear correlation between physical health and brain health.
Physical activity is any voluntary movement that requires energy. Aerobic exercise raises the rate of respiration and the heart rate. This boosts the immune system, reduces the risk of heart disease, type 2 diabetes, high blood pressure, and falls in older people. Most relevant to MAPP, it boosts cognitive function. Studies show that regular consistent exercise keeps the mind sharp and helps protect cognitive functions such as memory, thinking, and reasoning. Physical activity, especially strength-training, improves balance, increases neural functioning, and improves reaction time.
Many people often say that being in nature “clears our minds.” This is true, and there are also neurological reasons behind this. Recently, researchers studied more than 2,500 kids (ages 5-7). The researchers found that the children who spent more time outdoors had their memory improved by an average of 28 percent! They also found that children who spent time in nature were better at reading other people’s emotions and being socially aware due to increased an increase in brain activity.
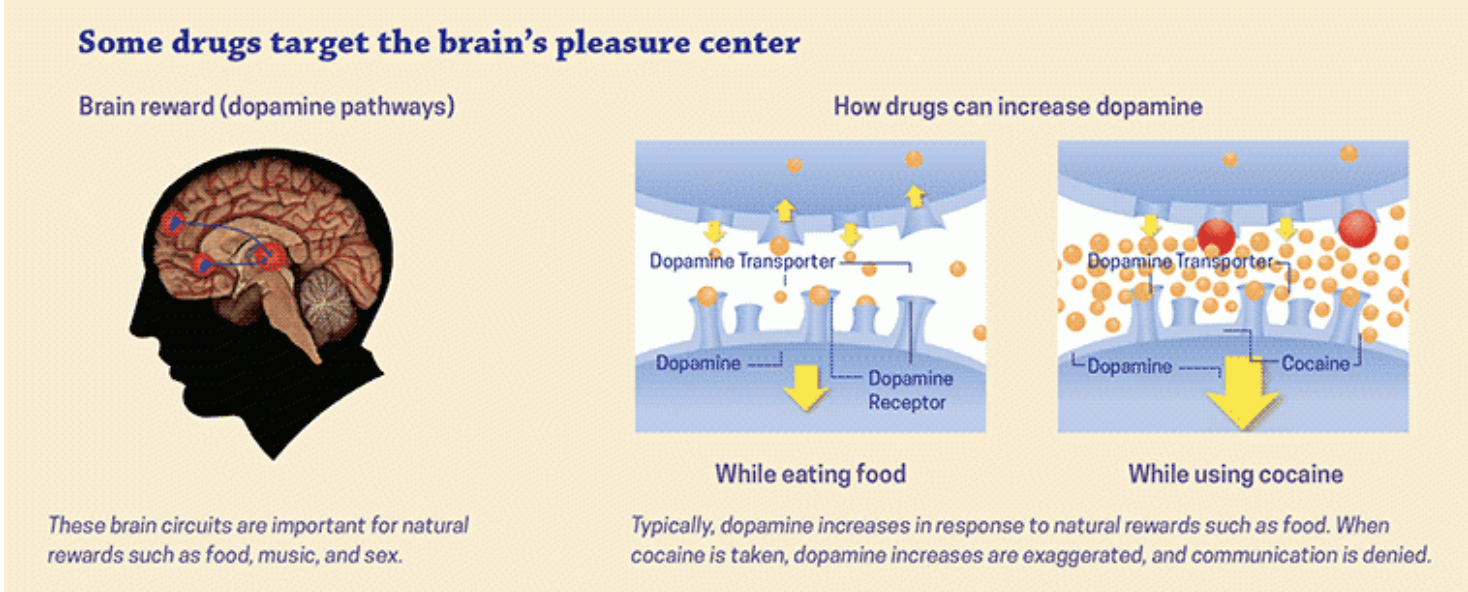
Exercise also boosts happy hormone and neurotransmitter levels! It boosts dopamine, noradrenaline, serotonin levels, and and serotonin levels, as well as GABA which is responsible for chemical messaging in the brain. The physical activity at camps also causes release of proteins that promote the growth of new neurons. In addition, the increase in blood flow during exercise causes the brain to receive more oxygen-rich blood, which increases the level of nutrients in the brain.
Exercise also increases molecular targets such as the brain-derived neurotrophic factor (BDNF). This increases synaptogenesis (synapse forming) making which makes it easier to absorb information and form long-term memories. Hence, the physical activity during summer camp summer that comes with a summer at camp significantly benefits the brain.
Decreased Screen Time:
In addition to increasing physical activity, most overnight camps are technology-free and thus decrease campers’ screen time. There’s nothing like seeing your phone on visiting day and finding hundreds of unread texts and notifications. In fact, reduced screen time changes the brain over time.
Early data from a landmark National Institutes of Health (NIH) study that began in 2018 indicates that children who spent more than two hours a day on screen-time activities scored lower on language and thinking tests. Additionally, some , and some children with more than seven hours a day of screen time experienced thinning of the brain’s cortex, which is related the area of the brain related to critical thinking and reasoning. Decreasing this screen time, however, prevents these adverse effects.
Decreased screen time is also correlated with better quality sleep. Screen time close to bedtime prevents bedtime bed time, prevents the increase in melatonin levels necessary to fall asleep. When sleep is decreased to less than seven hours, the brain has less time to clear beta-amyloid away, raising the risk of developing Alzheimer’s Disease. RBy reducing decreasing screen time can increase hours spent sleeping each night, which reduces this additional risk factor of developing Alzheimer’s Disease.
Camp & The Middle Prefrontal Cortex:
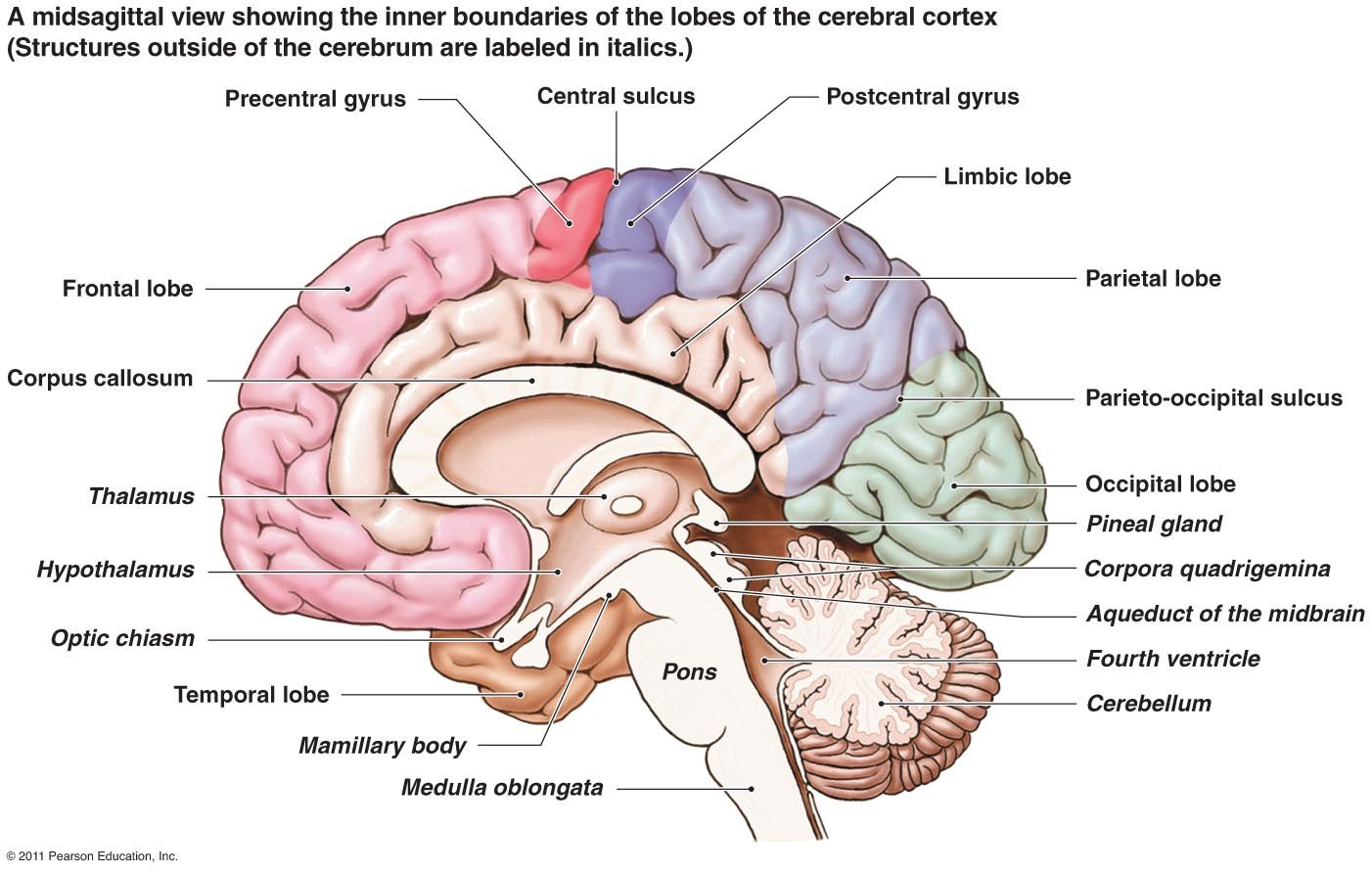
The middle prefrontal cortex is the front-most part of the frontal lobe and is found right behind the forehead. It serves various a variety of functions, and enables us to regulate our emotions, feel empathy, communicate, adapt to new situations, make good decisions, and overcome fear. It plays a prominent large role in maintaining and building relationships, and having good emotional and mental health.
When camps influence kids’ minds and make them more confident, build relationships with others, and become more independent, the campers’ mindsets/attitudes aren’t the only things that are changing; their they’re brain structure is actually changing as well, as the middle prefrontal cortex is forming new synapses.
Different experiences change the brain’s wiring writing of the brain through neuroplasticity when the brain creates new synapses (connections between neurons.) When kids have camp experiences that require them to be independent, form new relationships, and be flexible, these new synapses strengthen. Change in structure causes change in function, so the more these skills and habits are repeated, the more the synapses are strengthened, and the more these skills develop.
Conclusion:
Anyone who has spent a summer or two at sleepaway camp will likely tell you how it changed them. And while the summer did change them as a person, it also changed their brain structure and function. From increased physical activity to decreased screen time, and anatomical changes in the brain, such as in the prefrontal cortex, camp can have a significant great impact on our cognitive health.
Sources:
Cross, Jennifer, Dr. “What Does Too Much Screen Time Do to Children’s Brains?”
New York Presbyterian, healthmatters.nyp.org/
what-does-too-much-screen-time-do-to-childrens-brains/. Accessed 24 Apr.
2022.
Montemarano, Jada. “Youth anxiety and depression increased during pandemic;
summer camp could help.” Spectrum News 1, Charter Communications, July
2021, spectrumnews1.com/ca/la-west/health/2021/07/28/
youth-anxiety-and-depression-increased-during-pandemic–summer-camp-could-help#:~
:text=In%20addition%20to%20that%2C%20they,the%20mental%20health%20of%20kids.
Accessed 24 Apr. 2022.
“Summer Camp Boosts Brain Development.” nbc15.com, Gray Television, Inc., 27
Dec. 2018, www.nbc15.com/content/misc/
Summer-Camp-Boosts-Brain-Development-503576601.html. Accessed 24 Apr. 2022.
Bryson, Tina Payne, Dr. “Bunks Are Good for Brains: The Neuroscience of
Sleepaway Camp.” American Camp Association, American Camp Association,
Inc., Jan. 2014, www.acacamps.org/resource-library/camping-magazine/
bunks-are-good-brains-neuroscience-sleepaway-camp. Accessed 24 Apr. 2022.
“Give the Gift of the Outdoors: How Summer Camp Exercises Your Brain.” Camp
Kippewa for Girls, Scout Digital, kippewa.com/2020/01/30/
give-the-gift-of-the-outdoors-how-summer-camp-exercises-your-brain/.
Accessed 24 Apr. 2022.
“A Lack of Sleep in Middle Age Can Increase the Risk of Dementia.”
Healthline, Healthline Media, www.healthline.com/health-news/
a-lack-of-sleep-in-middle-age-can-increase-the-risk-of-dementia#How-the-brain-cle
anses-itself. Accessed 24 Apr. 2022.
Ruder, Debra Bradley. “Screen Time and the Brain.” Harvard Medical School, The
President and Fellows of Harvard College, 19 June 2019, hms.harvard.edu/
news/screen-time-brain. Accessed 24 Apr. 2022.